

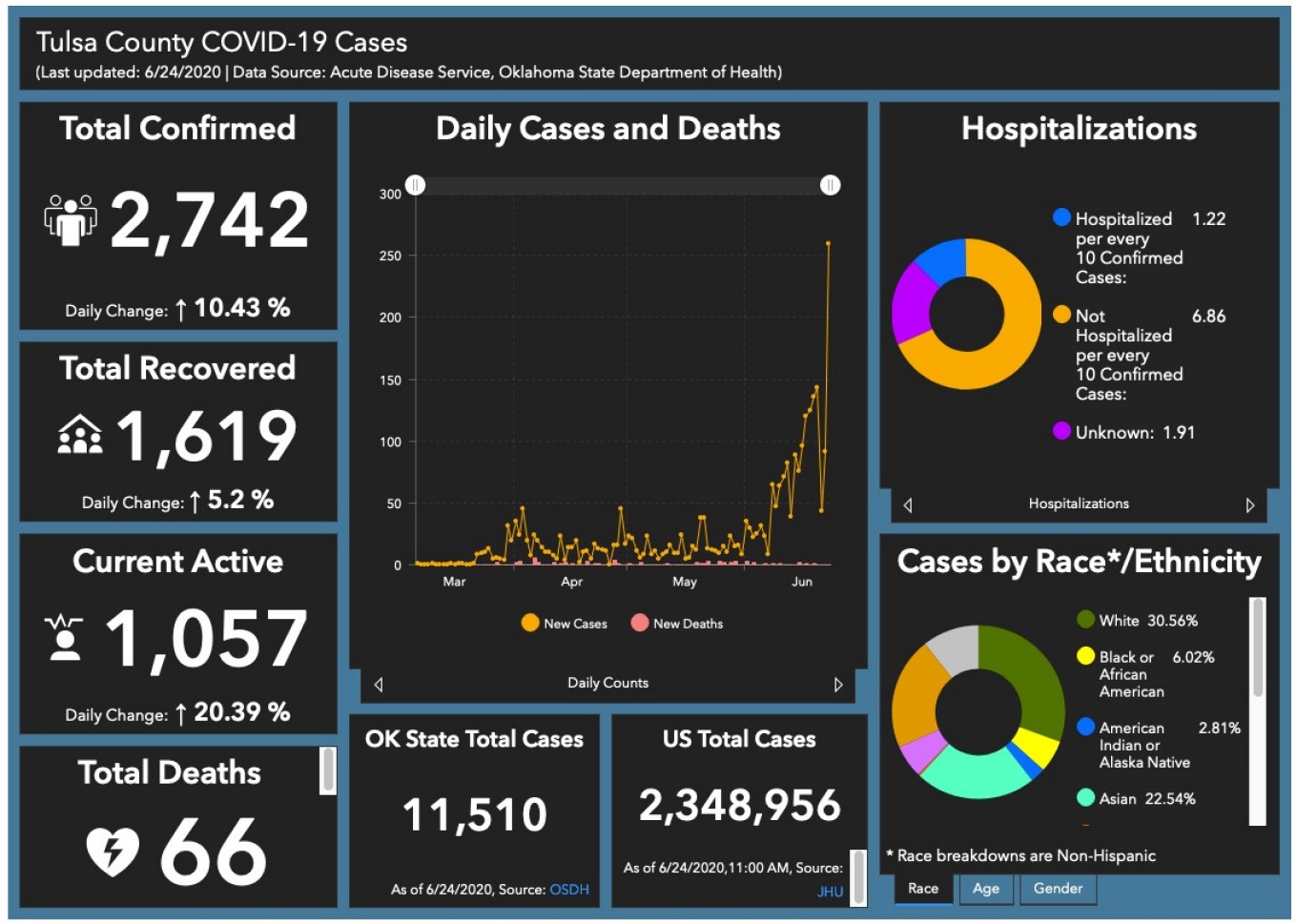

Tracking Tulsa County’s recent spike in COVID-19 Cases. Last updated: 6/24/2020 | Data source: Acute Disease Service, Oklahoma State Department of Health - https://www.tulsa-health.org/COVID19.
Published July 7, 2020 This content is archived.
BY MARCENE ROBINSON AND MICHELLE KEARNS
UB GSE doctoral student analyzes community virus data for Tulsa County, Oklahoma, as cases spike
Information science doctoral student crafts COVID-19 data models for government
Officials in Oklahoma are turning to information science doctoral student Monica Rogers for local COVID-19 data modeling. Rogers, who was recently promoted to division chief of data and technology for the Tulsa Health Department, has worked in information science for more than a decade. Before the outbreak, she forecasted community health needs and the prevalence of chronic conditions. Rogers now monitors COVID-19-related infections, hospitalizations and deaths, and makes data models that help inform county decisions. Most recently, her focus is tracking the sharp increase in cases for Tulsa County—including the city of Tulsa—and its population of 650,000. In late June, weekly case counts were double that of earlier in the month. By June 24, she tallied a county total of 2,742.


UB doctoral student and division chief of data and technology for the Tulsa Health Department, Monica Rogers analyzes data that helps local decision-makers craft guidelines for the community in Tulsa County, Okla.
While the rise is troubling, the death rate is relatively low, said Rogers. As of June 24, there had been 66 deaths since the first case was recorded in March.
“How many people are sick? How many will die? When will those things happen? These are the questions I try to answer in my models,” said Rogers. “We work with decision-makers to show different scenarios and their outcomes.”
The challenge with an infectious disease like COVID-19 is that information is constantly changing or doesn’t exist, said Rogers.
At the moment, Tulsa has re-opened and some aspects of life are starting to return to the way things were before the pandemic started. One noticeable difference: face masks are mandated for restaurant and bar employees. For now, they are the only people required to wear them. Large public events have returned. There has also been an influx of people who are not Tulsa County residents.
Fluxuations like these make modeling difficult, Rogers said. “We can’t use static variables from week to week.”
This means projections about future disease patterns are hard to make and it is difficult to use numbers to predict anything more than two weeks ahead.
“People should understand that we’re dealing with a new disease, so there are a lot of assumptions and a severe lack of good data. We’re assuming people are social distancing; we’re assuming people can’t get re-infected,” she said. “The earliest models have the widest ranges of potentials. It’s an iterative process. As we gain better data, we can tighten up projections so that they’re closer to reality.”
Rogers reviews and adjusts her projections each week knowing human behavior has the greatest influence on the spread of infection.
“Even if the model projected that the peak has already passed, that assessment was made with the assumption that people will continue to follow government guidelines,” said Rogers. “Models are not written in stone. They assume how people will behave. When their behavior changes, the model is no longer accurate.”
Rogers is optimistic that things will improve because municipal and health officials are committed to using data to make decisions. “That’s been extremely gratifying,” she said. “Decision makers are committed to being data informed.”
Tuesday News Briefs feature the stories of the Graduate School of Education faculty, students and alumni who are engaged in their communities and making an impact through their hard work, dedication and research initiatives. If you have a story to share, please email us with the details for consideration as a future news feature. | Email Us Your Story